Unified Patient Records from 16+ EMRs with MatchRite’s Common Data Engine
In episode 17 of Digital Health Hackers Podcast, Sidharth speaks to Christopher Jones, CEO of MatchRite Care, a patient-centered unified health record portal.
December 31, 2024
With over 20 years of experience in healthcare information technology, Christian Chevalley takes its challenges personally. Born in Geneva, Switzerland, Chevalley is now based in Thailand and tackles healthcare’s most pressing problem - its fragmented data sources. As a self-described ‘backend guy’, his solution is straightforward - to use the power of data infrastructure systems. It is after all, his life’s work.
Chevalley’s work has spanned industries, and he points out some stark differences - in the financial world the need to maintain a competitive edge and quick decision cycles provide a fertile ground for innovation. In contrast, healthcare technology innovation is not a budgetary priority and organizations need to be incentivized to adopt new technology.
Healthcare data is a source of much frustration and inspiration for Chevalley. His pursuit to connect fragmented data began with his early work with aged care facilities in Australia and the US. The burden on care workers is immense and having easy access to resident information at the point of care would be of some reprieve. However, building comprehensive patient histories involves communicating with numerous legacy databases.
In similar interactions with an ophthalmology practice based in the US, Chevalley was tasked with building a custom solution to replace an existing monolithic EHR. “As IT guys we oversimplify [problems],” Chevalley says, and we agree. In these interactions, the true complexity of healthcare systems came to light - and understanding this complexity is essential to enabling practitioners in providing patient-centric care.
Learning to interface with the many existing legacy systems became a critical part of the problem. Moving all of this data to standardized systems like openEHR is a long road, and with severely limited technology budgets, puts the cart before the horse.
Another common approach is mapping legacy data to modern structures, which is limited by loss of information and cumbersome maintenance. And so a problem statement emerged - how do we leverage data trapped in silos with the least amount of pain and overhead?
Around this time Chevalley encountered openEHR, which at first seemed daunting and hard to implement. With his team he explored existing libraries and several open source options to implement an openEHR based healthcare data management system. In the initial years, the explorations bore few results.
In parallel, database systems were evolving with PostgreSQL adding JSONB as a data type in 2014. This marked a new era in relational databases allowing for the storage of unstructured data without having to incorporate NoSQL databases. etherCIS was born of this premise.
Released in 2016, etherCIS Clinical Data Repository was one of the first open source openEHR implementations and had Chevalley at its helm as the lead developer. It was enterprise-grade, vendor-neutral, allowed complex querying through the Archetype Query Language (AQL), and exposed its services via a RESTful API. An early implementation was done in Leeds, England in an open platform Person Held Record.
By 2019, EHRbase emerged as a successor to etherCIS and eventually replaced it. It was developed by Vitagroup, in collaboration with HiGHmed and Hanover Medical School Germany.
Ever since, Chevalley has had a clear vision of where the solutions to healthcare’s data woes lie - in the capabilities of the database layer. The more common and computationally intensive solution to accessing information from varied legacy databases is to create an API layer that takes care of interactions. This is a tricky affair, inefficient on large datasets, and error-prone due to the many APIs and query dialects that need to be employed.
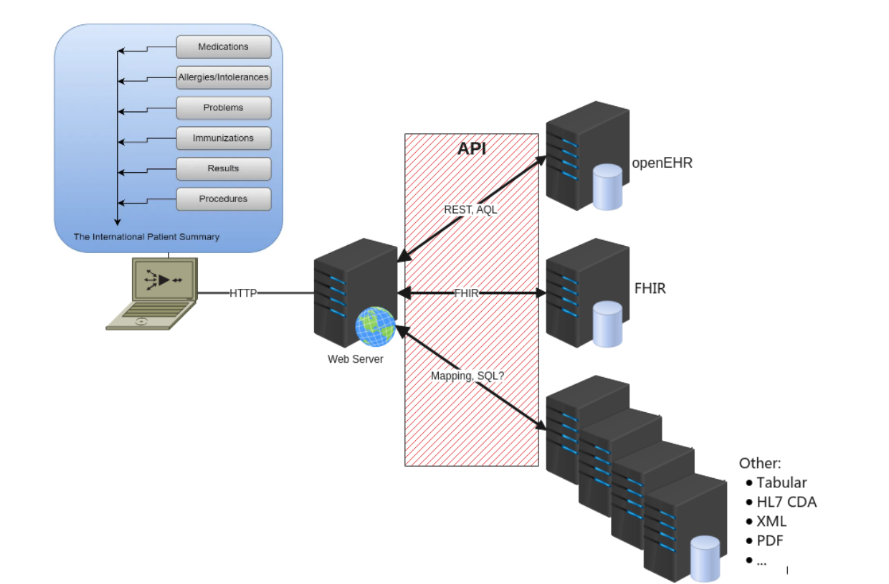 Querying many databases is often performed through an API layer
Querying many databases is often performed through an API layer
Why then, is it still preferred by many developers? Many developers avoid working with databases, often dismissing it as boring or legacy technology. “Databases are really powerful tools that need to be used to the max,” says Chevalley, “SQL theoretically can deal with any computational problem [with features like] recursion, loops and control structures.”
Without reinventing the wheel, a simpler solution can be built using the database management system capabilities available today. Chevalley’s latest endeavor, titled etherCIS3 per this whitepaper, does just that.
Chevalley’s proposed model is an extensible, scalable, and secure clinical data platform that enables format-agnostic data capture and federates heterogeneous clinical data. He proposes replacing the API layer by a common service able to manipulate data sources regardless of format. With transactions performed via Domain Specific Language (DSL), this approach easily supports cross platform querying.
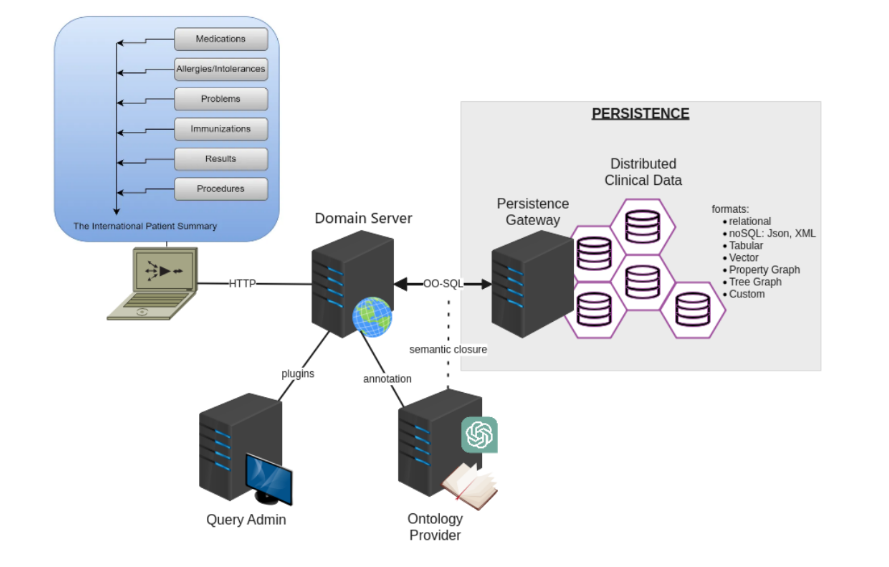 Chevalley’s proposed solution
Chevalley’s proposed solution
Inspired by a seminal study illustrating this approach, Chevalley’s proposed architecture extensively leverages PostgreSQL Foreign Data Wrappers (FDW). The FDW creates foreign data tables that can then be accessed as the primary database. It supports a persistence implementation through this approach.
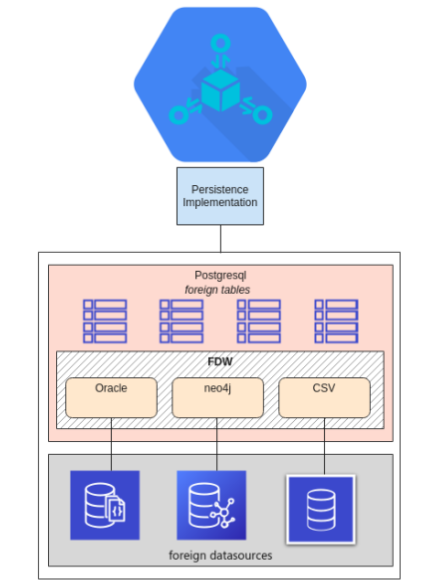
Chevalley’s proposed solution supports a persistence implementation through the use of PostgreSQL’s FDW
Several architectural patterns are used in order to ensure scalability, extensibility, and reliability such as event sourcing, Domain Driven Design, and Command Query Responsibility Segregation. The platform kernel is hence based on the Hexagonal architecture design pattern - separating applications into ‘inside’ containing core logic and ‘outside’ containing databases, UI, messaging queues, etc.
The core or domain kernel in this case, instantiates plugins and parallelizes routing requests and responses. Plugins are designed to process specialized functions according to the separation of concerns pattern, implementing only a specific use case (e.g. FHIR resource capture, business logic, etc.) Plugins also conform to the Shared Nothing Architecture, limiting contentions between plugins and the core module.
Plugin invocation and orchestration is based on a concurrent actor model in order to support parallelism in query execution, load balancing, fallback strategies, and operating concepts such as live upgrades. A detailed architecture diagram is included below.
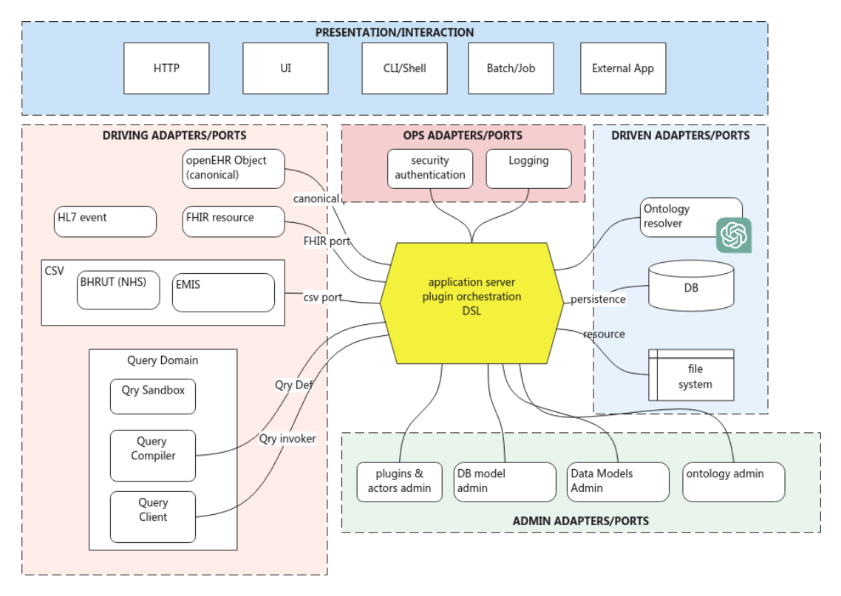 Detailed architecture diagram
Detailed architecture diagram
The DSL extends Java Object Oriented Querying or jOOQ to make it possible to access value points without specifying complex path expressions. This is enabled by a query engine with a high level of abstraction implemented using simple algorithms. This approach handles data types and their representations, joins, and even prevents SQL injection at the database level, thus making it simpler for application designers (Like us! Check out how we’re reinventing the EHR with Medblocks UI).
As Chevalley put it, “Write a sh*t ton of SQL” to get things done.
A limitation of this approach is the need for careful storage planning – making external databases available via FDW can be storage intensive.
The next step for etherCIS3 would be to implement a proof of concept. Chevalley places the development in the test and refine phase, with an emphasis on the core concepts - the framework must remain flexible and extensible.
A potential area where powerful impact can be made by federating heterogeneous clinical data is in distributed healthcare systems in rural areas. Working with existing data infrastructure to generate comprehensive patient profiles and journeys available at the point of care would be a compelling win.
It’s an exciting time in the healthcare data space when etherCIS mastermind Christian Chevalley is back with new, disruptive ideas. The secret to his success seems to lie in embracing and experimenting with the latest technological innovations. With his new proposal titled etherCIS3, Chevalley introduces ways to work with existing legacy data systems by leveraging the capabilities of modern database management systems. “Postgres is the Linux of databases,” he says, and we’re inclined to believe him.
Watch the complete interview with Christian Chevalley at our Digital Health Hackers Podcast here
Legacy systems, disconnected data, and complex integrations—what is holding your organization back? Reach out to us to explore how Medblocks and our network of experts could be a part of your solution.
In episode 17 of Digital Health Hackers Podcast, Sidharth speaks to Christopher Jones, CEO of MatchRite Care, a patient-centered unified health record portal.

In episode 15 of Digital Health Hackers Podcast, Sidharth speaks to Prof. David Ingram, one of the creators of openEHR, exploring his innovation journey.

In conversation with Dr. Videha Sharma, CEO of Fava Health, Sidharth discusses the future of precision medicine and the technology infrastructure needed.
No comments yet. Be the first to comment!