




If you’ve ever wondered what the early days of openEHR looked like, this story is for you. Learn how an unlikely band of academics, clinicians and engineers, led by the vision of Professor David Ingram, sparked the global openEHR movement.
By the age of 30, Professor David Ingram had a grounding in math and computer science, a first degree in theoretical physics, a PhD in biomedical engineering and several years of work experience in designing and managing complex engineering projects. Social care was a core aspect of his family history and personal experience as well, as for the first 12 years of his life, he grew up in a residential children’s home run by his parents.
In the first volume of his book, Health Care in the Information Society, he says “And as the poet wrote about taking paths less travelled, it did make all the difference” in reference to his wide explorations during his early career. His journey is testament to the strength of perspective that an interdisciplinary mindset can bring to driving sustainable innovation - in his case, to developing the leading healthcare open standard of our time, openEHR.
Prof. David Ingram with his book, Health Care in the Information Society
Early professional experiences#
In 1976, Prof. David Ingram was appointed a lecturer and founding member of an experimental department of medical informatics in London’s St. Bartholomew Hospital, in a “new-fangled discipline of linking the computer with medicine” as he puts it. He worked under John Dickinson (1927-2015) who he describes as a “courageous and far-sighted academic Chief of Medicine at Bart’s” in his book, who was also his PhD co-supervisor. Here he tried to translate his perspectives of modelling weather patterns into modelling the human body, including the circulatory system, respiratory dynamics, fluid and electrolyte exchange and pharmacokinetics.

St Bartholomew's the world's oldest hospital, was founded in 1123
Taking this to “a thousand institutions around the world” they realized that the data environment in healthcare was not at the time conducive to the same mathematical modelling approach that you may successfully use with the weather system. In weather, you can model the physics of the components, whereas in medicine, context is all. Paraphrasing Prof. Ingram, it wasn’t ‘feasible or tractable’ to model in the healthcare domain at the time.
He also did several stints that exposed him to the wider world of healthcare, connecting him to his social care background and interests. He worked in medicine education and computer resources with the Marie Curie Foundation, producing a series of interactive video disks which profiled cancer patients and their families. Soon, his career included more involvement with conceptualizing and creating the vision of a healthcare record.
The Good European Health Record or GEHR project#
The GEHR project was a precursor to openEHR, working towards creating a coherent information architecture for the digital healthcare record. It was initiated in 1991 by Dr. Alain Maskens, a Belgian oncologist and Dr. Sam Heard, an Australian GP, as a consortium led by Prof. David Ingram to bid on electronic health record architecture with the EU Advanced Informatics in Medicine (AIM) Initiative.
“One of the great things in this space is you have to have something to start with, to incrementally experiment with it, and see where it falls short to improve it,” and the product developed by Dr. Maskens’s company, HDMP, served as this starting point. The GEHR project was completed and submitted in 3 months and was enthusiastically endorsed. The project officially began in January 1992 in spite of opposition from companies that hoped to productize and earn from the healthcare domain.
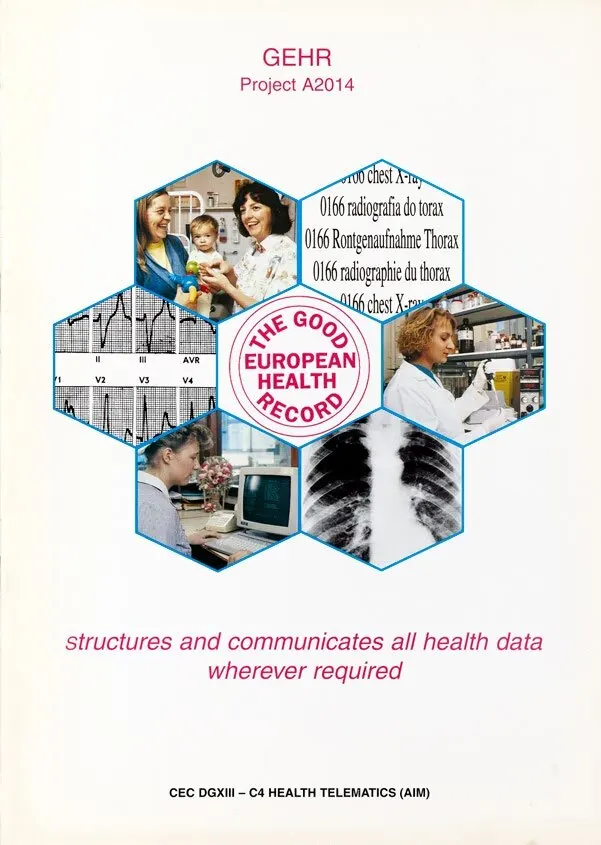
Front sheet of the GEHR Project Brochure, 1994
Pioneering the two-level modelling paradigm#
It was after this that the two-level modelling paradigm came into being. Prof. David Ingram and Dr. Jo Milan (from the Royal Marsden Hospital, London) joined a new consortium to implement Synapses, a project focused on federated EHR integration. Here the new dual-model approach was introduced, separating EHR structure from clinical context using an object dictionary for consistency.
In 1996, these efforts were reinvigorated by Dr. Sam Heard and Tom Beale, designing the GEHR Archetype System that refined the two-level modelling approach, involving both record architecture and clinical standards. “Having something to eat,” as Prof. David Ingram put it was ensured by representing these innovations in conversations with the European Commission and evaluating the monetary losses created by a data environment that operated in silos and didn’t communicate well.
Trillions of dollars have been lost to disparate health IT ecosystems#
Healthcare systems have a tendency to localize. Each care system - a clinic or a department - has, to an extent, their own way of doing things. And while there is a case to be made for specialized systems that cater to very localized requirements, the information and monetary loss that comes from this approach is massive. In switching different vendors to meet specific requirements, and academic projects running out of funding streams, it’s easy to make the case that trillions of dollars have been lost to healthcare IT, recording information that is not available to us today.
Solving this was a primary intention of the Original openEHR Manifesto, and it was an important initiative to make this available in the public domain as well, in order to achieve the scale that healthcare needs. Having seen 5 eras of replacing data in healthcare institutions, Prof. David Ingram has first-hand experience of how data is lost from implementation to implementation. His mission and vision have always been clear. Especially in designing healthcare for the future, common standards of communication become a necessary foundation in order to enable greater connectedness and flexibility.
From openEHR to open care#
Medical Nemesis, a book written by Ivan Illich in 1975 describes what could be called a “radical” approach to the future of healthcare. Paraphrasing an idea from the book, Prof. David Ingram says “I foresee a future where the only stuff medicine will do, will be stuff the patient can manage in their own hands.” During the interview, Dr. Sidharth Ramesh, founder of Medblocks, agrees, citing glucose monitoring machines as an example of technology-enabled, patient-empowered care. Sidharth then raises an interesting question about what is lost with the approach of patient care being within the domain of a doctor.
“They are both right, because it’s personal choice,” responds Prof. Ingram, highlighting an important aspect about the future of care. “Not everyone is going to be an e-Patient Dave, going into that level of detail … but other people passionately do.” He has also been a vocal advocate for designing an organic care information utility that can accommodate much more input and interaction with the experience of the individual patient. He describes it to be organic in contrast with the inflexibility of machines, and the rigidity that the design of IT systems requires. What would the data systems that accommodate this level of flexibility look like? Can common, standardized healthcare data systems be designed without standardizing healthcare processes?
Do medical process need to be standardized?#
Prof. Ingram quotes a common adage in the healthcare domain, “if you have 6 doctors, you’ll have 7 opinions”. Interestingly, Jordi Piera, the Director of Digital Health Strategy for Catalonia, mentioned this phrase in his conversation with Sidharth as well. There are several healthcare processes that have shown to benefit from standardization, such as the Advanced Trauma Life Support or ATLS protocol followed in A&E departments and Dr. Gawande’s books on healthcare improvement.
However rather than seeing this as a trend towards more standardization, Professor Ingram says it’s “horses for courses.” That is, use standardization where it is advantageous rather than setting it up as an absolute principle. The conditions in which healthcare is required and delivered are variable according to local context and culture. The hope he expresses is that IT systems remain agile enough to remain a good partner in this journey.
When Sidharth asks him about his perspective on AI, he says, “It’s a slightly misleading umbrella term of ‘intelligence’ … which is far from the underlying reality.” Knowing the mathematical foundation of the models changes his perspective, “some of it is just basic statistics,” he says. All statistical models require robust data to be trained on. Could AI be the answer to providing flexible yet standardized technological support to healthcare? I’d go back to Prof. Ingram’s opinion on standardization, “horses for courses”, finding the use cases where AI can provide benefits vs seeing it as a one-size-fits-all solution.
Recording the history of healthcare information systems#
To know more about Professor David Ingram’s fascinating journey and insights into the healthcare information systems world, his books, Health Care in the Information Society, Vol I and II, published in 2023 are a great place to start. In its preface it says “The book has been written as a postscript to a career spent in exploring, supporting and connecting many and disparate interdisciplinary and multiprofessional endeavours.” By drawing extensively on first-hand experiences, his books attempt to tell the story of healthcare’s experiments with information technology. They’re available on-demand in print form, and for free digitally by the Open Book Publishers.
In his incredible journey Professor David Ingram has traversed through theoretical physics, complex system engineering and academia before co-founding one of the leading healthcare standards of today, openEHR. His interdisciplinary approach and unique perspective have been crucial to the unique and robust approach that openEHR carries, one of collaboration, innovation and continuous learning in community.
Early projects such as GEHR and Synapses, and alliances with innovators such as John Dickinson, Dr. Alain Maskens, Dr. Sam Heard, Jo Milan and Tom Beale, incrementally built the ideas that were later formalized as openEHR. openEHR’s unique two-level modelling approach and archetype structure allow the flexibility required by implementations that cater to local cultures and requirements while allowing standardization and adherence to a common language. Even within the realm of standardization, Prof. Ingram’s philosophy is simple, use it where it is appropriate. That makes sense.
Understanding the journey today's systems and standards have taken to reach their present form can be essential towards enriching your knowledge. Watch this podcast episode between Sidharth and Professor David Ingram to catch the details of their discussion.
Have you been exploring different health standards and experimental approaches towards having IT support your complex health workflows? Attend our free workshop hosted by Dr. Sidharth Ramesh to answer your burning openEHR questions, or to go beyond the basics and into implementation.