Archetypes and Templates Explained
In the previous module, we looked at why data platforms are needed and difficult to build. The applications, while they need expressivity and they want to represent all the data that’s needed for their use case, it’s also important for these apps to interoperate and reuse the data where they can.
One issue is semantic variation. Different platforms or vendors may model the same concept, say, blood pressure or tumor staging in incompatible ways. Even if data can technically be exchanged, inconsistent meanings lead to misinterpretation, duplication, or loss of important clinical context. Hospitals want to tailor data capture to their workflows, but interoperability requires adherence to agreed models. This often leads to trade-offs between flexibility for local use and consistency across systems.
openEHR solves this in a rather elegant way.
Archetypes as clinical models
Archetypes are maximal clinical models that are modeled separately from the data platform itself but these archetypes also use the same data types that are initially referenced in the RM.
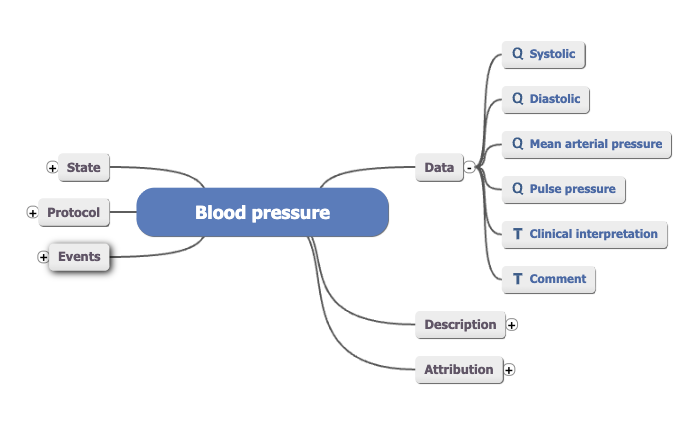
Archetypes are a big asset of openEHR, there are close to a 1000 different archetypes in the CKM. They capture the meaning, structure, and limitations of clinical concepts; things like blood pressure, lab results, or a diagnosis.
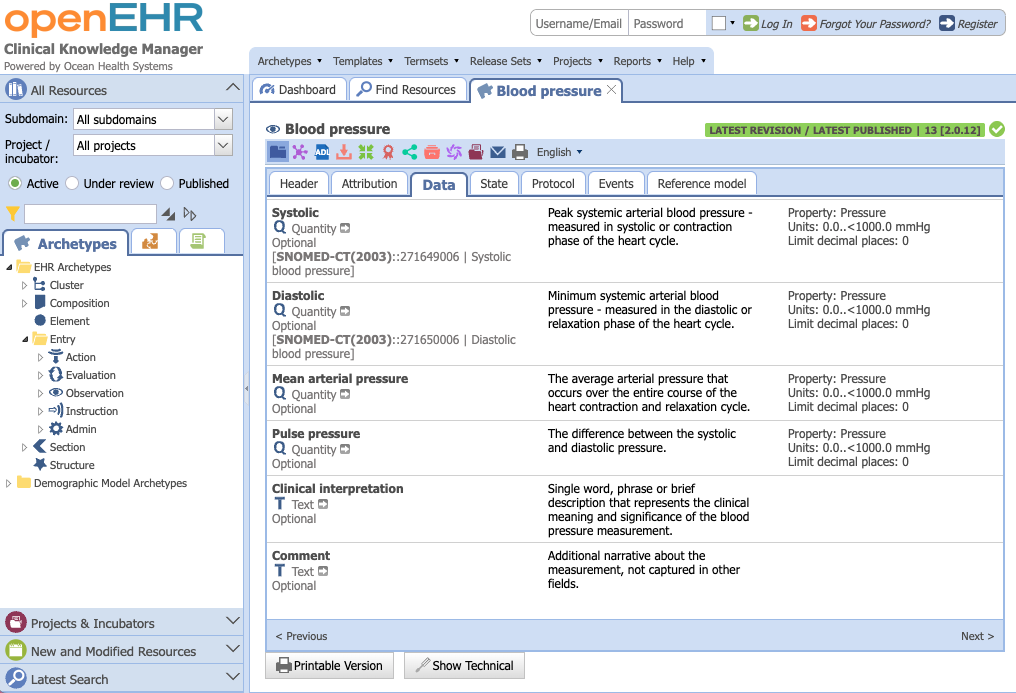
An archetype is a standardized, community-agreed specification of a clinical concept. For example, a “Blood Pressure” archetype defines that it must include systolic, diastolic, units of measurement, and the time of recording.
Together with the openEHR Reference Model, archetypes enable semantic interoperability. This means a blood pressure recorded in one system can be reliably understood and reused in another, because both follow the same clinical model.
The role of templates
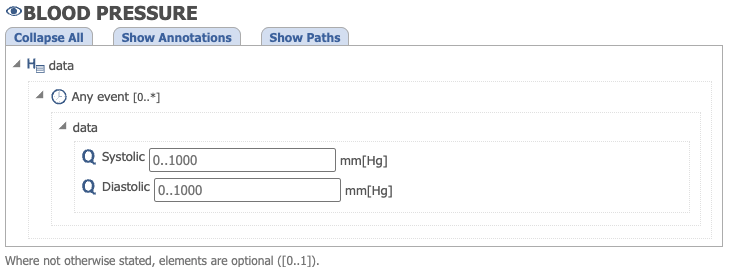
While an archetype defines one clinical concept, a template bundles several archetypes to reflect how clinicians actually record data in practice, such as an admission note or lab request form.
Templates act as the bridge between application and the data platform. Applications use templates to generate user interfaces and APIs, while the data platform stores and validates the data according to those same templates.
Because templates can be tailored for local workflows without changing the underlying archetypes, they allow hospitals to customize data entry while preserving interoperability. In effect, templates connect the needs of applications with the stability of the platform, making data usable both clinically and technically.
This blood pressure template, for example, only includes systolic and diastolic values and excludes other data points.
Understanding data model contracts for interoperability
When there are no clinical models, the data platforms have no idea about what can be captured, but since this is defined outside, each application can decide for itself what data fields or archetypes it wants to use. This is usually done through clinical modeling.
Once an archetype is defined, different applications can reuse it for their own purposes. For example, if one application wants to capture a blood pressure reading during an outpatient visit, it can use the Blood Pressure archetype. Another application, perhaps for inpatients where BP is recorded daily, can also use the same archetype. Because both use the same model, the data is consistent and interoperable.
Hence, it’s really important to understand these contracts.
The data platform itself only knows about the basic rules of the Reference Model. Archetypes are built separately, based on the Reference Model, and then fed into the platform. Once inside, they act as contracts that guide applications on how to capture and exchange information. This reuse of archetypes is what makes interoperability between applications possible.
In the next lesson, we’ll have a look at the openEHR CKM (Clinical Knowledge Manager) where these Archetypes and Templates are stored.