Archetype Deepdive: Capturing Family History and Lifestyle Risks
In the previous lesson, we captured why the patient came in for a consultation. This includes the story and the presenting problem, which gives us a good starting point.
To expand the initial clinical assessment template, let’s revisit the scenario.
Revisiting the clinical scenario
We are modelling a patient’s initial clinical assessment. This involves capturing:
- the current issue
- patient narrative
- family history
- lifestyle factors like alcohol consumption and smoking history
- vital signs
After understanding the patient’s main complaint, the doctor often asks broader questions to understand context.
- “Does anyone in your family have medical problems?”
- “Do you smoke?”
- “Do you drink alcohol?”
The answers to these questions involve patient input, but are not recorded as is. They often need clarification, interpretation and sometimes calculation.
To record this type of information, we go from OBSERVATION to EVALUATION.
Observation vs Evaluation
At a high level,
- OBSERVATION is used when information is recorded directly from the patient
- EVALUATION is when the clinician applies judgement to gather information
For example, the patient’s story, or a questionnaire they fill out will be OBSERVATIONs, whereas family history and lifestyle habits are EVALUATIONs. You can refer to this earlier lesson on the openEHR Reference Model for more details.
Capturing family history
If we search the openEHR Clinical Knowledge Manager (CKM) for “family” we will see more than one result.
Based on our clinical scenario, we will choose the family_history.v2 archetype.
To do this, let’s think about what information we need to capture. There are two broad ways in which family history can be captured.
The first way is through using screening questions. For example, you give the patient a list of predefined conditions such as diabetes, hypertension, and heart disease. In this case, the patient checks yes or no, or says that they don’t know. In that case, you record answers directly from the patient without any interpretation.
For this, you would use an OBSERVATION.
The second way is when the doctor is talking to the patient, asking follow-up and clarifying questions, and potentially looking at previous medical documents. Based on all this information, the clinician forms a judgement about family history.
In this case, you would use an EVALUATION, as the clinician interprets and summarizes information.
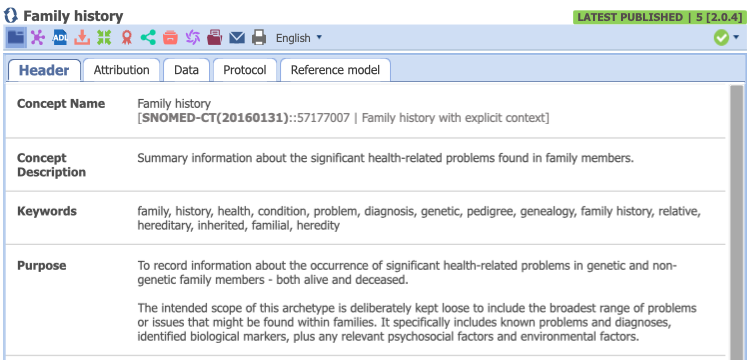
Exploring family_history.v2
If you look at the ‘Purpose’ of family_history.v2 you’ll see that it’s meant to record a summary of significant health-related problems in family members, both living and deceased.
This aligns well with how family history is taken in practice, so let’s add this archetype to the template. You can use the panel on the bottom-right for searching for and adding archetypes.
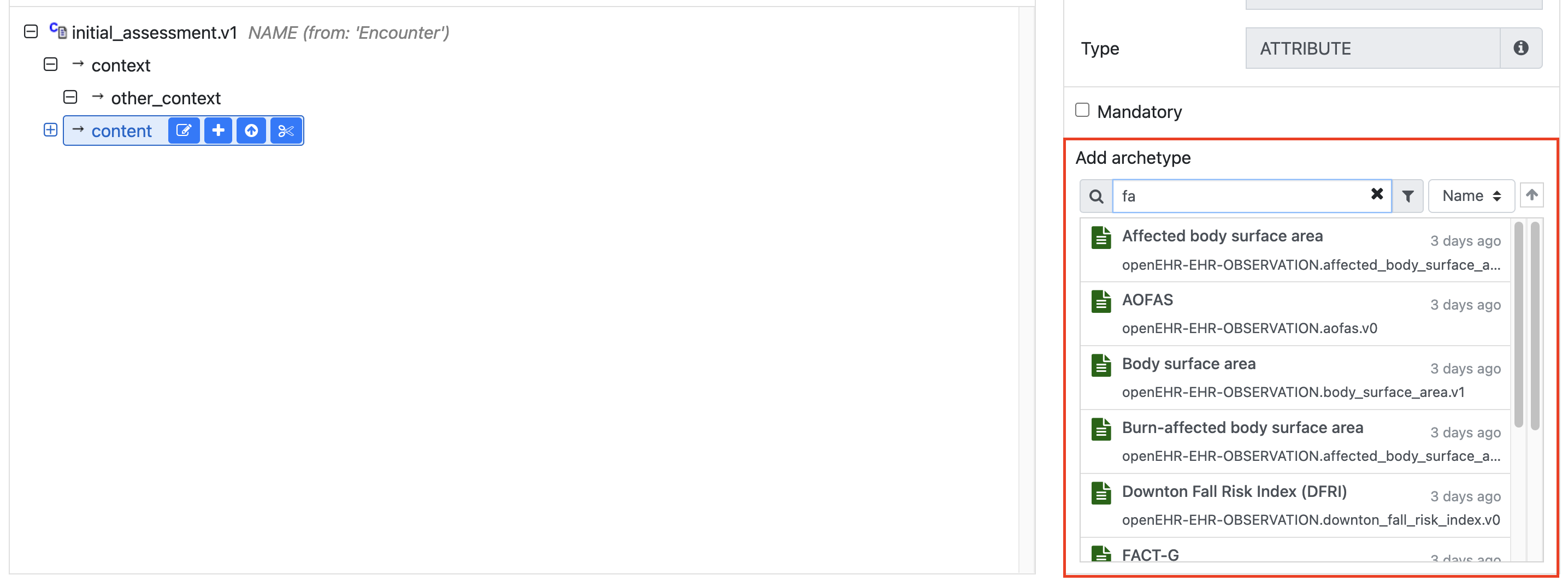
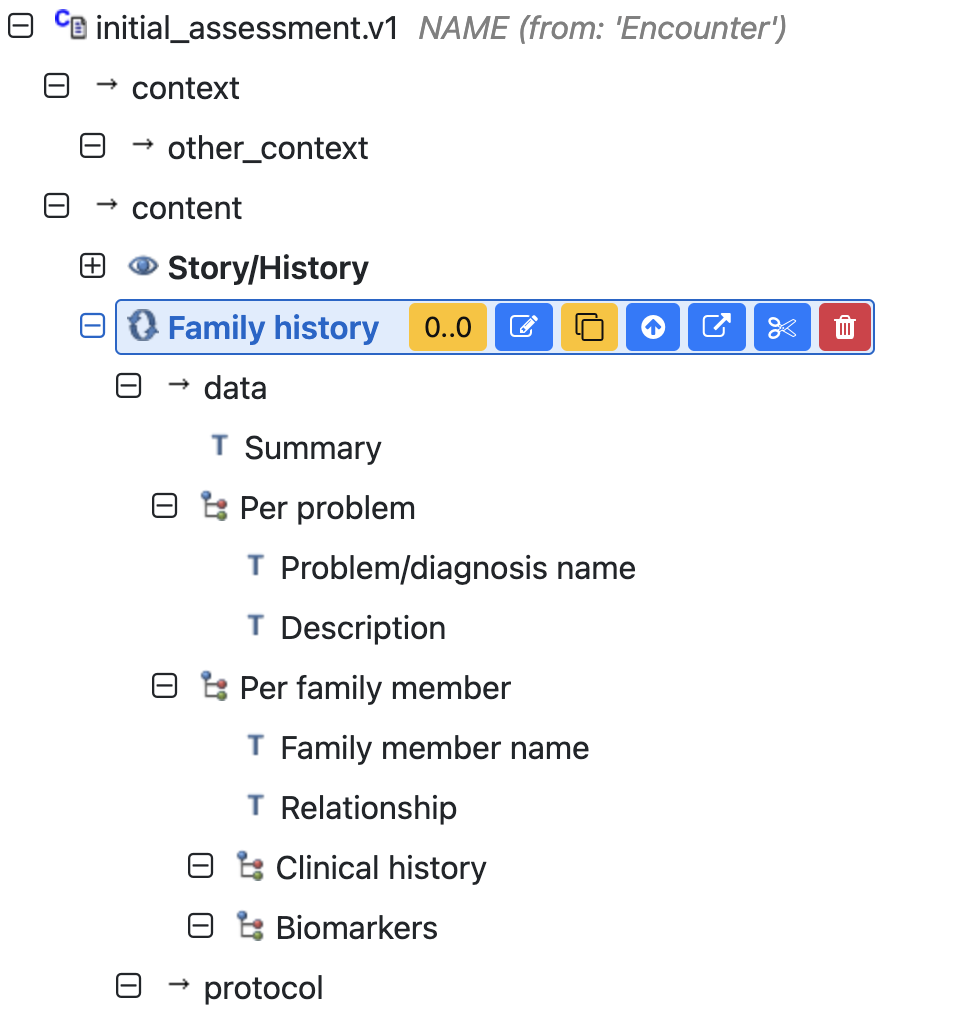
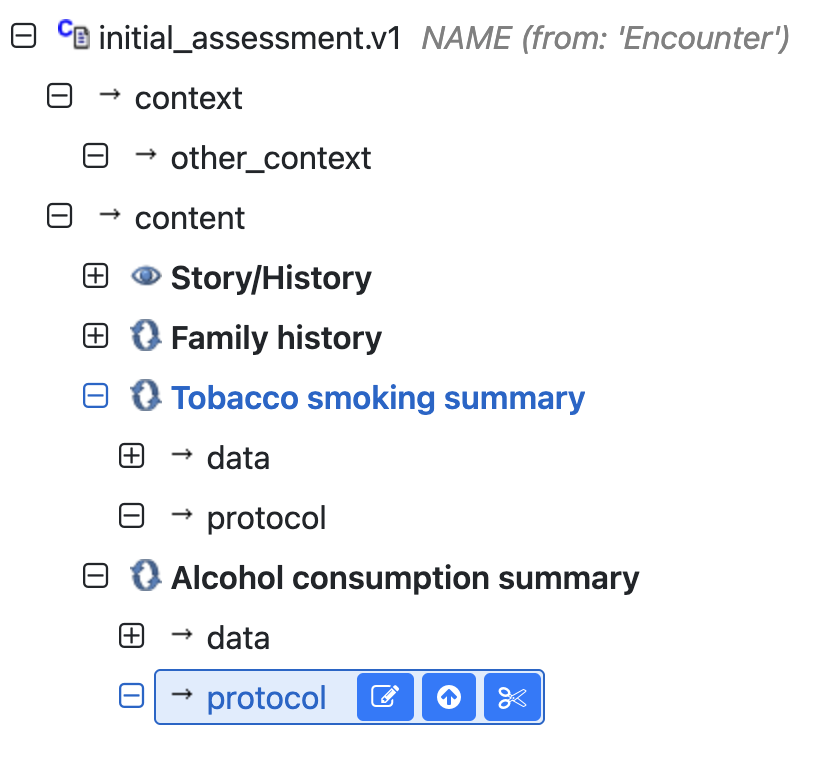
This is how the template would look after adding the archetype.
Capturing lifestyle factors
The next two pieces of information we want to capture are the patients smoking and drinking habits. If we search for that in the CKM, we will find the following archetypes:
Exploring tobacco_smoking_summary.v1
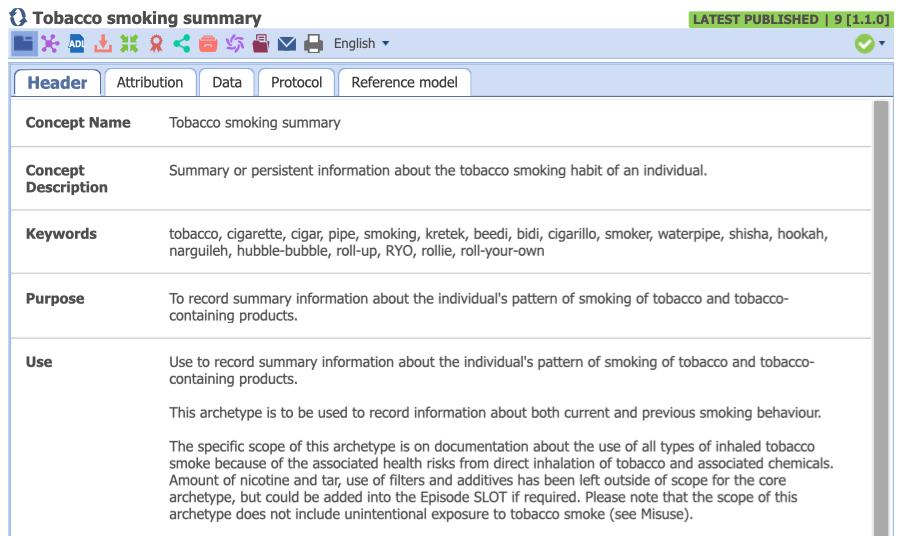
In this archetype, details such as current status and duration of smoking, as well as calculated values like pack years are to be captured. The presence of a calculated field, and the additional clinical judgement required to capture information clearly makes this an EVALUATION.
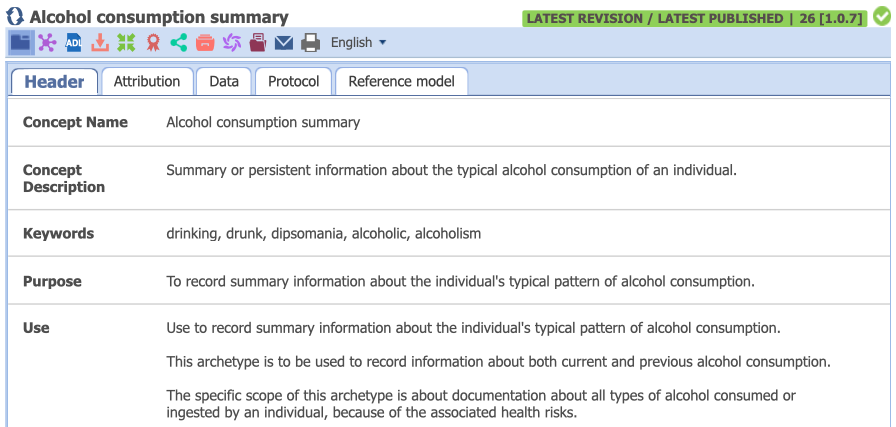
Exploring alcohol_consumption_summary.v1
The alcohol consumption summary also includes fields that are captured based on the clinician’s judgement, including patterns of consumption, current drinking status, start and end dates, attempts made to quit drinking etc. Even though this information is gathered from the patient, the clinician has to interpret and summarize it.
We can now add both archetypes to our template.
Lesson summary
At this stage, our initial assessment template captures the patient’s story and presenting complaint, family history, smoking history and alcohol consumption history. These are the first few steps followed in this clinical scenario.
This lesson is also about understanding when judgement is involved in the clinical workflow. It is not necessary to memorise what archetypes are available, rather the skill to develop is to evaluate and select appropriate archetypes as required.
